ANTITHROMBOTIC PROPHYLAXIS RECURRENT PREECLAMPSIA
IN PATIENTS WITH THROMBOPHILIA
Zhuravleva E.V., Bitsadze V.O., Makatsariya A.D.
Дата публикации на сайте: 2015-10-30 Доступна также в печатной версии журнала Резюме | Полный текст | Скачать в PDF
Акушерство, гинекология и репродукция. 2015; N3: c.28-34
Резюме:
Objective. To evaluate the efficiency of antithrombotic therapy to prevent repeated preeclampsia in patients with thrombophilia. Subject and methods. A prospective clinical study was conducted 66 patients with thrombophilia (genetic, acquired or concomitant) and with history of preeclampsia: 35 patients addressed and were followed since fertile cycle (subgroup Ia) aObjective. To evaluate the efficiency of antithrombotic therapy to prevent repeated preeclampsia in patients with thrombophilia. Subject and methods. A prospective clinical study was conducted 66 patients with thrombophilia (genetic, acquired or concomitant) and with history of preeclampsia: 35 patients addressed and were followed since fertile cycle (subgroup Ia) and 31 patients addressed during pregnancy and were followed since 6-13 weeks of gestation – IIa subgroup. Control group – 50 patients without both obstetrics and gynecology and thrombotic complications in history. Therapy included LMWG (Enoxaparinum natrium), B vitamins, antioxidants and micronized progesterone. Results. The all period of pregnancy, obstetric and perinatal outcomes were better in patients receiving therapy since fertile cycle compared with group of patients whose therapy was initiated during pregnancy. Conclusion. To prevent re-PE at a subsequent pregnancy, the therapy should be start since fertile cycle, continuing during pregnancy, childbirth and the postpartum period. Therapy should include LMWH, B vitamins, antioxidants and micronized progesterone.
DOI: 10.17749/2070-4968.2015.9.3.028-034
Abbreviations: AFD – antenatal fetal death; ADP – adenosine diphosphate; AKA – anticardiolipin antibodies; AT III – antithrombinIII;
APA – antiphospholipid antibodies; APTT – activated partial thromboplastin time; LA – lupus anticoagulant;
INR – international normalized ratio; LMWH – low molecular weight heparins; PE – pre-eclampsia; IUGR – intrauterine growth retardation; TAT – thrombin-antithrombin complexes; TEG – thromboelastography; APC – activated protein C;
PAI-1 – activator inhibitor plasminogen-1.
Received: 28.08.2015; in the revised form: 10.09.2015; accepted: 27.09.2015.
Conflict of interests The authors declared that they do not have anything to disclosure regarding funding or conflict of interests with respect to this manuscript.
All authors contributed equally to this article.
For citation Zhuravleva E.V., Bitsadze V.O., Makatsariya A.D. Antithrombotic prophylaxis recurrent preeclampsia in patients with thrombophilia. Akusherstvo, ginekologiyaireproduktsiya / Obstetrics, gynecology and reproduction. 2015; 3: 28-34 (in Russian).
АНТИТРОМБОТИЧЕСКАЯ ПРОФИЛАКТИКА ПОВТОРНЫХ ПРЕЭКЛАМПСИЙ У ЖЕНЩИН С ТРОМБОФИЛИЕЙ
Журавлева Е.В., Бицадзе В.О., Макацария А.Д.
ГБОУ ВПО «Первый МГМУ имени И.М. Сеченова» Минздрава России, Москва
Резюме Цель исследования – оценка эффективности противотромботической профилактики повторных ПЭ у женщин с тромбофилией. Материалы и методы. Проведено проспективное клиническое исследование с участием 66 пациенток с тромбофилией (генетической, приобретенной или сочетанной) и ПЭ в анамнезе: 35 – обратившиеся и, соответственно, находящиеся под нашим наблюдением с фертильного цикла (подгруппа Ia), и 31 – обратившиеся к нам, уже будучи беременными (с 6 по 13 нед. гестации) – IIa подгруппа. Контрольную группу составили 50 женщин с неотягощенным акушерско-гинекологическим и тромботическим анамнезом. Терапия проводилась НМГ, витаминами группы В, антиоксидантами и микронизированным прогестероном. Результаты. У пациенток, получавших терапию с фертильного цикла в течение беременности, акушерские и перинатальные исходы были лучше, чем в группе пациенток, терапия которым была начата во время беременности. Заключение. Для предотвращения повторной ПЭ при последующей беременности необходимо начинать терапию с фертильного цикла, продолжая во время беременности, родов и в послеродовом периоде. Терапия должна включать НМГ, витамины группы В, антиоксиданты и микронизированный прогестерон.
Ключевые слова Преэклампсия, антитромботическая профилактика, НМГ, тромбофилия.
Статья поступила: 28.08.2015 г.; в доработанном виде: 10.09.2015 г.; принята к печати: 27.09.2015 г.
Конфликт интересов Авторы заявляют об отсутствии необходимости раскрытия финансовой поддержки или конфликта интересов в отношении данной публикации.
Все авторы сделали эквивалентный вклад в подготовку публикации.
Для цитирования Журавлева Е.В., Бицадзе В.О., Макацария А.Д. Антитромботическая профилактика повторный преэклампсий у женщин с тромбофилией. Акушерство, гинекология и репродукция. 2015; 3: 28-34.nd 31 patients addressed during pregnancy and were followed since 6-13 weeks of gestation – IIa subgroup. Control group – 50 patients without both obstetrics and gynecology and thrombotic complications in history. Therapy included LMWG (Enoxaparinum natrium), B vitamins, antioxidants and micronized progesterone. Results. The all period of pregnancy, obstetric and perinatal outcomes were better in patients receiving therapy since fertile cycle compared with group of patients whose therapy was initiated during pregnancy. Conclusion. To prevent re-PE at a subsequent pregnancy, the therapy should be start since fertile cycle, continuing during pregnancy, childbirth and the postpartum period. Therapy should include LMWH, B vitamins, antioxidants and micronized progesterone.
First Moscow State Medical Sechenov University of the Ministry of Health Russian Federation
Introduction
In the modern obstetrics practice the socially significant issue is the obstetric complications leading to the pregnancy termination, as well as to increased level of perinatal and maternal mortality [7]. PE – preeclampsia – is a pathological condition associated with pregnancy and characterized by hypertension and proteinuria after 20 weeks of gestation, appearing in about 4% (1.5 to 10%) of all pregnancy cases and being one of the leading causes of maternal and fetal morbidity and mortality [11]. PE is the most important cause of perinatal morbidity and mortality in the world [8,9,10]. The risk of perinatal mortality in this disease increases 5-fold [16]. It is thought that PE is a cause of 75,000 maternal deaths worldwide annually [6]. Broadening and extension of knowledge on the modern means of PE prevention deserves close attention.
In 1980ies-1990ies there was a series of discoveries of multiple genetic forms of thrombophilia, including FV Leiden mutation, prothrombin mutation G20210А, polymorphisms of the genes controlling fibrinolysis system -PAI-1, 4G/5G, polymorphisms of tissue-type plasminogen activator t-РА I/D, of fibrinogen 455 A/G, of factor XII etc, as well as antiphospholipid syndrome (APS) [12,13]. The studies began for the role of hyperhomocysteinemy in the development of atherothrombosis and venous thromboembolism. Simultaneously the researchers began to study the role of genetic and acquired thrombophilia in the ethiopathogenesis of not only thrombotic but also of typically obstetric complications - preeclampsia, miscarriages, fetal growth retardation syndrome (FGR), antenatal fetal death (AFD), premature detachment of normally located placenta, that determine the perinatal morbidity and mortality [2,4,5]. According to the data of the studies of the group headed by Professor A.D. Makatsaria, as well as the worldwide literature data, such obstetric complications as PE and fetal loss syndrome are associated with multigene and combined forms of thrombophilia in 70-77% of cases [3,7,14,15]. Currently the results of meta-analysis allow us to separate the genetic and acquired forms of thrombophilia into the independent group of risk factors for primary obstetric complications (PE, fetal loss syndrome, fetal growth retardation syndrome etc.) [17]. Due to this fact the scientific community is now facing the need to search the new form of prevention of recurrent pregnancy complications, including PE.
A number of scientists, such as Rey Е., Gamen Р., Fait G., Many A., Kupfermink MJ., Gris JC., Brenner B. made such attempts and got very optimistic results.
The objective of our work is the evaluation of anti-thrombotic prevention of recurring PE in the women with thrombophilia.
Materials and methods
We examined 66 patients with thrombophilia (genetic, acquired or combined) and PE in their medical history, who were included in the prospective group: 35 patients with PE in anamnesis who addressed and respectively was followed up by us since the start of fertile cycle (Ia subgroup), and 31 patients with PE in anamnesis who addressed us when already pregnant (week 6 till week 13 of gestation) – IIa subgroup. Patients in Ia subgroup were examined and consulted before pregnancy and were followed up during the entire gestation period after the delivery. The patients in subgroup IIа were evaluated before the pregnancy (as a part of retrospective group); however they were followed up only since the moment of their address to us (when already pregnant, on terms 6 to 13 weeks).
The control group consisted of 50 women with uncomplicated pregnancy course, uncomplicated obstetric-gynecological and thrombotic anamnesis.
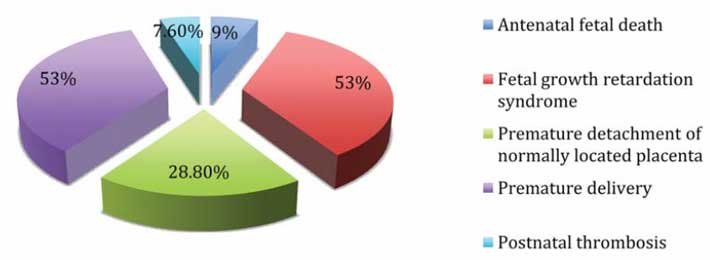
The Figure 1 shows the obstetric anamnesis of the patients from the prospective group.
Figure 1. Obstetric anamnesis of the patients from the prospective group.
The diagram data show the following: the most frequent obstetric pathology in this group of patients were fetal growth retardation syndrome and premature delivery: in 35 patients (53%), the second most frequent – premature detachment of normally located placenta – in 19 patients (28.8%), antenatal fetal death was in anamnesis of 6 patients which constituted 9%, thromboses in the postnatal period were detected in anamnesis of 5 patients (7.6%).
Regardless of the hemostasis defect type, all the patients received the basis therapy with anti-thrombotic drugs (starting from fertile cycle in groupIa, from the moment of address in group IIa). – Aspirin (Thrombo-ASS 25-100 mg) depending on the platelets function, LMH – Fraxiparine or Clexane in the dose 0.3-0.9 ml QD subcutaneously (since the start of the pregnancy in groupIa, since the moment of address in group IIa). As the part of the additional therapy all the patients in the prospective group were given group B vitamins (Multitabs В complex), folic acid no less than 4 mg per day as part of basis therapy (in the patients with hyperhomocysteinemia caused by the MTHFR mutation), polyunsaturated fatty acids (Omega 3, Omega 6).
Before the LMH prescription the USI was performed on mandatory basis in order to:
Clarify the uterine localization of the gestation sac
Lack of the chorionic exfoliation sites
Also before the Fraxiparine prescription, and then 10 days after this and then once per month we performed the control of the level of thrombophilia markers ТАТ, D-dimer, measured the level of homocysteine in plasma, protein C function (Parus-test), level of PAI-1, aggregation platelets activity. This is necessary to select the adequate drug dose and to control the effectiveness and safety of the drug use. The group of the patients displayed progesterone insufficiency (the possible cause for it being APLA circulation), due to which they all were given Utrogestan (200-800 per os and vaginally) up to week 24 of pregnancy. In case of lack of blood secretions the vaginal use of the drug is preferable – it leads to rapid absorption, primary passage through endometrium, decreased concentration in general blood flow and lack of the systemic effect on the early pregnancy term. Regarding aspirin, it is prescribed depending on the circulation of APA-cofactors for polymorphism of platelets receptors and aggregation platelets activity in the mini-doses of 75 mg/day. Both Fraxiparine and aspirin were prescribed as part of the basis therapy, starting from fertile cycle (in case of presence of high levels of thrombophilia markers), duration and doses of the drugs were adjusted depending on the degree of the risk of thrombotic complications.
LMH was taken subcutaneously 1-2 times per day continuously during the entire pregnancy. The day before the cesarean section the drug was discontinued in order to prevent the hemorrhagic complications, and 8 hours after the surgery the therapy was restored for 10 days, with the duration of the therapy subject to change – depending on the condition of the hemostasis system parameters. Tests used for the evaluation were as follows: APTT, thromboelastography, prothrombin time.
Results
Table 1 shows the results of the baseline evaluation of hemostasis system in the patients from prospective group.
Table 1. Results of baseline evaluation of hemostasis system in the patients of prospective group.SD – standarddeviation.
Parameters
Prospective group (n=66)
Control group (n=50)
APTT (sec), mean±SD
27.3±3.1
27.1±0.5
Prothrombin time (sec), mean ± SD
103±7.5
101±11.7
Thrombin time (sec), mean ± SD
18±1
17.1±2.3
Fibrinogen (g/l), mean ± SD
4±0.5
3.5±0.3
АТ III, mean±SD
112.5±20
114.8±20
r+k (sec), mean ± SD
19±3
21±0.5
ma (mm), mean±SD
50±3.2
47.5±2.8
ITP (CU), mean ± SD
33±4
28±2
Platelets aggregation with ADP 1х10^3 M(%),mean±SD
51±5
38±2
Platelets aggregation with ristomycin 1×10^3 M(%), mean ± SD
50±3
40±1.5
APC resistance (“Parus Test”), n(%)
5 (7.6%)
1 (2%)
D-dimer (µg/ml), mean ± SD
2.1±0.5
0.5±0.5
Also before the LMH prescription we performed the study of the thrombophilia disorders structure in the patients from prospective group (Table 2).
Table 2. Structure of the thrombophilia disorders in the patients of prospective group before the treatment with LMH.
Parameters
Patients of prospective group, n=66
D-dimer
35 (53%)
ТАТ
38 (57.5%)
ВА (+)
10 (15.2%)
Homocysteine
11 (16.7%)
Anti-beta-2-GP-1
12 (18.2%)
Anti-prothrombin antibodies
8 (12%)
Anti- annexin V
5 (7.6%)
АКА
25 (37.9%)
PAI-1
35 (53%)
Aggregation activity
41 (62.1%)
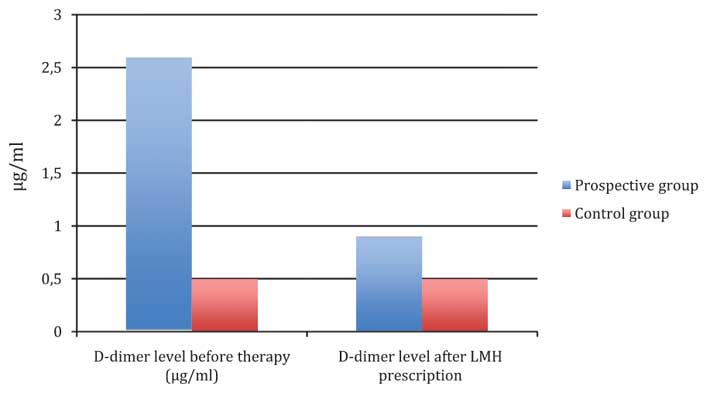
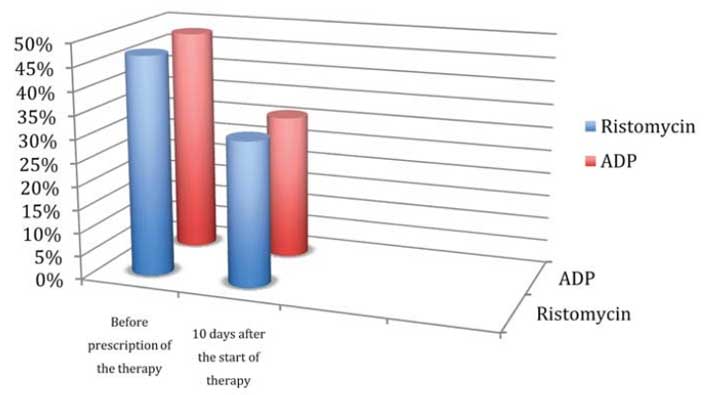
Thus the parameters of hemostasiogram of the studied patients showed the following changes: increased D-dimer was noted in more than a half of the patients (53%), increased level of TAT complex was noted in 57.5%, aggregation activity of platelets was noted in 62.1%, ВА was noted in 10 patients – 15.2%, increased PAI-1 level was noted in 53% of cases. No patients displayed increased hemorrhagic tendencies. 5 patients with the medical history including the thrombosis in postnatal period had the relatively higher levels of those markers due to which they were prescribed higher doses of LMH. With this therapy at III trimester the marker levels in the patients of prospective group were comparable to the ones of the patients in the control group. Let us review this dynamics in example of D-dimer (Figure 2), as well as aggregation activity of platelets (Figure 3).
Figure 2. Dynamics of D-dimer level after LMH prescription (on day 10).
Figure 3. Dynamics of platelets aggregation activity after prescription of the therapy (on day 10).
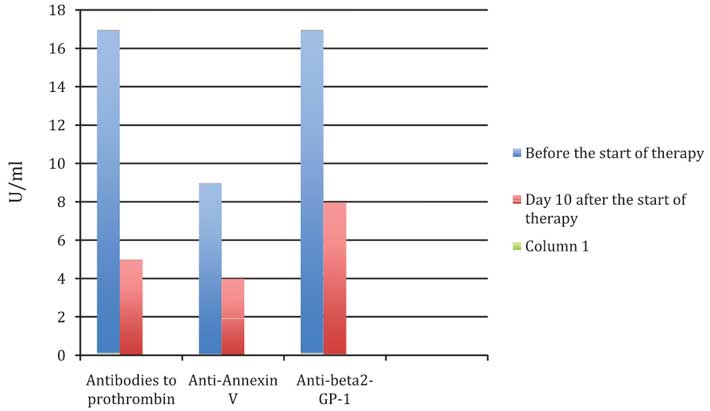
Also after LMH prescription there was noted the decrease in the levels of APA-cofactors, levels of prothrombin antibodies, anti-annexin V, anti-beta-2GP-1 (Figure 4). That was also the dynamics regarding homocystein.
Figure 4. Dynamics of the decrease in AFA-cofactors levels in the patients of prospective group during the therapy.
Apart from the monitoring of laboratory data the patients in the prospective group underwent the control of therapy efficiency using clinical functional methods as well. For example, in order to evaluate the condition of uteroplacental and fetoplacental blood flow on term 30-32, 34-36 and 38 weeks there was performed USI with Doppler velocimetry.
As the result the course and the outcome of pregnancy in this group of the patients were the following (Table 3): fetal growth retardation syndrome was noted in 7 patients out of the group, in 2 patients from the subgroup Ia and in 5 patients from subgroup IIa. The threat of pregnancy termination in the prospective group of patients was noted in 6 (9.1%): 1 (2.9%) and 6 (16.1%) in subgroups Ia and IIa, respectively. The premature delivery was not observed in any patients in subgroup Ia, in subgroup IIa it was observed in 2 (6.5%), and no patients in control group had premature delivery. The urgent cesarean section was not performed to any patient: neither in prospective group nor in the control group. Regarding the gestation toxicosis: mild gestation toxicosis was observed in the patients in Ia, IIa and in control group- 1 (2.9%), 6 (16.1%) and 5 (10%), respectively. Data distribution for the moderate gestation toxicosis: 0, 2 (6.5%), 0, respectively. We were able to prevent severe PE, while the moderate PE was observed only in 2 patients in IIa group, neither Ia subgroup nor control group had the PE cases.
Table 3. Structure of complications of course and outcome of pregnancy in the patients of prospective group.
Parameter
Prospective group
Control group (n=50)
SubgroupIa, n=35
SubgroupIIa, n=31
Total, n=66
Fetoplacental blood flow disorder IA
1 (2.9%)
4 (13%)
5 (7.6%)
1 (2%)
Fetal growth retardation syndrome
2 (5.7%)
5 (16.1%)
7 (10.6%)
2 (4%)
Gestation toxicosis, n (%)
1 (2.9%)
6 (16.1%)
7 (10.6%)
5 (10%)
-Mild
1 (2.9%)
4 (13%)
5 (7.6%)
5 (10%)
-Moderate
0
2 (6.5%)
2 (3%)
0
PE
0
2 (6.5%)
2 (3%)
0
- Moderate
0
2 (6.5%)
2 (3%)
0
- Severe
0
0
0
0
Threat of pregnancy termination, n (%)
1 (2.9%)
5 (16.1%)
6 (9.1%)
5 (10%)
Premature delivery, n (%)
0
2 (6.5%)
2 (3%)
0
Cesarean section, n(%)
35 (100%)
31 (100%)
66 (100%)
12 (24%)
Urgent cesarean section, due to the critical condition of mother/fetus, n (%)
0
0
0
0
Thus we can see that the number of obstetric complications was significantly higher in the subgroup of the patients follow-up of which started when they were already pregnant and not in fertile cycle (unlike subgroup Ia).
All the patients delivered via cesarean section. In the control group only 12 (24%) patients delivered via cesarean section, mostly elective one: due to high degree of myopia, scar on the uterus after the cesarean section surgery, pelvic presentation of fetus.
66 live children were born, with mean weight 3,250±250 g, height 51±2 cm, Apgar score 75%- 8-9 points and 25%- 7-8 points. Early neonatal period was unremarkable.
Regarding the further follow-up and the therapy of the patients from prospective group: the day before the surgery LMH drugs were discontinued with the therapy resumed 8 hours after surgery. It shall be noted that LMH doses varied depending on the thrombotic history of the patients: in case of complicated anamnesis the patients were given the drugs in the dose 0.6-0.9 ml, in uncomplicated anamnesis – 0.3 ml. In a month the patients were transferred to Warfarin, the duration of therapy course was 6 months (target INR 2.0-3.0).
All the patients were followed up in the early and late postnatal period, there was performed the analysis of clinical symptoms and control of molecular markers of thrombophilia. On day 8-10 post surgery the values of those markers decreased just like the parameters of inopexia. Thrombohemorrhagic complications (postnatal hemorrhage, hematometra, subinvolution of uterus) were not detected in any of the patients, also there was no difference in the volume of blood loss between the patients from prospective and control groups, just like in the necessity of blood transfusion, which indicates the safety of LMH use during pregnancy and in postnatal period.
The data shown above (Table 4) make it evident that the early start of LMH therapy in the patients of prospective group allowed us to achieve the perinatal outcome, statistically comparable to the ones in the control group. All the patients had the uncomplicated pregnancy course and the favorable perinatal outcomes. Thus we can deduce that for the optimized follow-up of the next pregnancy and the possibility of the timely start of the adequate preventive therapy, all the patients with PE in anamnesis need to perform the study of hemostasis system for genetic and acquired thrombophilia form.
Table 4. Perinatal outcomes in the patients from prospective group and control group.
Parameter
Prospective group
Control group (n=50)
SubgroupIa, n=35
SubgroupIIa, n=31
Total, n=66
Antenatal fetus death, n (%)
0
0
0
0
Live birth, n, (%)
35 (100%)
31 (100%)
66 (100%)
50 (100%)
Weight at birth (g), mean ±SD
3,250(±250)
3,250(±250)
3,250(±250)
3,350(±505.5)
8-9 points
29 (83%)
20 (65.5%)
49(75%)
38 (76%)
7-8 points
6 (17%)
11 (34.5%)
17(25%)
12 (24%)
≤6 points
0
0
0
0
Necessity of transfer to specialized neonatal care in-patient facility, n(%)
0
0
0
0
Conclusions
All the patients with PE in anamnesis need to be tested for thrombophilia (acquired and genetic).
Detection of thrombophilia (acquired, genetic or combined) in the patients with PE in anamnesis gives us the possibility for pathogenetic justification of effective prevention of this complication in subsequent pregnancies.
In order to prevent the repeated PE in subsequent pregnancy one need to start the therapy from fertile cycle, continuing it during the pregnancy, childbirth and in postnatal period. Therapy shall include LMH, group B vitamins, antioxidants and micronized progesterone.
Discontinuation of LMH 24 hours before the planned cesarean section and resuming the therapy 8 hours after the surgery allowed us to avoid hemorrhagic and thrombotic complications in 100% of cases.
References
Alfirevic Z., Roberts D. et al. How strong is the association between maternal thrombophilia and adverse pregnancy outcomes. A systematic review. Eur. J. Obstet. Gyn. Reprod. Biol. 2002; 101 (1): 6-14.
Baimuradova S.M. Pathogenesis, principles of diagnosis and treatment of the syndrome of fetal loss due to acquired or genetic defects and hemostasis. Dr. diss. Moscow. 2007; 396 s.
Bitsadze V.O. Pathogenesis, principles of diagnosis and prevention of complications of pregnancy, due to thrombophilia. Dr. diss. Moscow. 2004; 251 s.
Brenner B., Hoffman R., Blumenfeld Z. et al. Gestational outcome in thrombophilic women with recurrent pregnancy loss treated by enoxaparin. Thromb. Haemost. 2000 May; 83 (5): 693-7.
Cervera R., Piette J.C., Font J. et al. Euro-Phospholipid Project Group. Antiphospholipid syndrome: clinical and immunologic manifestations and patterns of disease expression in a cohort of 1,000 patients. Arthritis Rheum. 2002. Apr; 46 (4): 1019-27.55.
Dossenbach-Glaninger A., van Trotsenburg M., Dossenbach M. et al. Plasminogen activator inhibitor 1 4G/5G polymorphism and coagulation factor XIII Val34Leu polymorphism: impaired fibrinolysis and early pregnancy loss. Clin. Chem. 2003 Jul; 49 (7): 1081-6.
ris J.C., Mercier E., Quéré I. et al. Low-molecular-weight heparin versus low dose aspirin in women with one fetal loss and a constitutional thrombophilic disorder. Blood. 2004 May 15; 103 (10): 3695-9.
Kovac M., Mitic G. et al. Thrombophilia in women with pregnancy-associated complications: fetal loss and pregnancy-related venous thromboembolism. Gynecol. Obstet. Invest. 2010; 69 (4): 233-8.
Main E.K. Maternal mortality: new strategies for measurement and prevention. Curr. Opin. Obstet. Gynecol. 2010 Dec; 22 (6): 511-6.
Makatsariya A.D., Bitsadze V.O., Akin'shina S.V. Thrombosis and thromboembolism in obstetric practice. 2007; 151 s.
Makatsariya A.D., Bitsadze V.O., Smirnova L.M., Akin'shina S.V., Baimuradova S.M. Thrombohemorrhagic complications in obstetric practice. Guidance for doctors Moscow. 2011; 1056 s.
National Institute for Clinical Excellence. Why Women die. Report on Confidential Enquiries into Maternal Deaths in the United Kingdom, 1997-1999. London. 2001.
Pandey M., Mantel G.D., Moodley J. Audit of severe acute morbidity in hypertensive pregnancies in a developing country. J. Obstet. Gynecol. 2004; 24: 387-391.
Saving Mothers. Third Report on Confidential Enquiries into Maternal Deaths in South Africa 2002-2004. Department of Health, Pretoria.
Villar J., Abalos E., Nardin J.M., Merialdi M., Carroli G. Strategies to prevent and treat preeclampsia: evidence from randomized controlled trials. Semin. Nephrol. 2004; 24 (6): 607-15.
About the authors
Zhuravleva Ekaterina Viktorovna – MD, PhD, research associate of the Ob/Gyn Department of The First Moscow State Medical Sechenov University. Address: ul. Trubetskaya, 8, str. 2, Moskva, Russia, 119048. Tel.: +7(495)788-58-40. E-mail: evyashenina@list.ru
Bitsadze Victoria Omarovna – MD., Professor, Department of Obstetrics and Gynecology, Faculty of Medical and Preventive, First Moscow State Medical Sechenov University. Address: ul. Trubetskaya, 8, str. 2, Moskva, Russia, 119048. Tel.: +7(495)788-58-40. E-mail: gemostasis@mail.ru.
Makatsariya Aleksandr Davidovich – MD, corresponding member of the Russian Academy of Sciences, Professor, Head of the Department of Obstetrics and Gynecology, Faculty of Medical and Preventive, First Moscow State Medical Sechenov University. Address: ul. Trubetskaya, 8, str. 2, Moskva, Russia, 119048. Tel.: +7(495)788-58-40. E-mail: gemostasis@mail.ru.
Сведения об авторах
Журавлева Екатерина Викторовна – к.м.н., научный сотрудник кафедры акушерства и гинекологии МПФ Первого МГМУ им И.М. Сеченова. Адрес: ул. Трубецкая, 8, стр. 2, Москва, Россия, 119048. Тел.: +7(495)788-58-40. E-mail: evyashenina@list.ru.
Бицадзе Виктория Омаровна – д.м.н., профессор, профессор кафедры акушерства и гинекологии медико-профилактического факультета Первого МГМУ им. И.М. Сеченова. Адрес: ул. Трубецкая, 8, стр. 2, Москва, Россия, 119048. Тел.: +7(495)788-58-40. E-mail: gemostasis@mail.ru.
Макацария Александр Давидович – д.м.н., член-корреспондент РАН, профессор, заведующий кафедрой акушерства и гинекологии медико-профилактического факультета Первого МГМУ им. И.М. Сеченова. Адрес: ул. Трубецкая, 8, стр. 2, Москва, Россия, 119048. Тел.: +7(495)788-58-40. E-mail: gemostasis@mail.ru.